

Surgical Strategies in Timing of Cholecystectomy in the Elderly
Surgical Strategies in Timing of Cholecystectomy in the Elderly
Debating Cholecystectomy in Elderly Patients: Balancing Timing for Optimal Outcomes

In this debate, two contrasting studies regarding cholecystectomy timing in elderly patients with biliary pancreatitis with/without ERCP were published this year. They present divergent strategies, sparking discussions on whether immediate surgery or delayed intervention is more advantageous. In this multifaceted debate, one study advocates for a wait-and-see strategy post-ERCP in elderly patients with common bile duct stones, emphasizing the safety of deferring cholecystectomy after successful stone removal. Contrarily, another study favors early cholecystectomy in frail geriatric patients with acute biliary pancreatitis, showcasing the benefits of immediate surgical intervention in reducing complications, readmissions, and mortality rates compared to non-operative management followed by unplanned cholecystectomy. Both studies highlight the complexity of patient management decisions and stress the importance of individualized care based on nuanced clinical judgment and comprehensive patient evaluation.
Wait-and-see strategy is justified after ERCP and endoscopic sphincterotomy in elderly patients with common biliary duct stones.1 This study focused on elderly patients (75 years or older) who underwent endoscopic stone extraction but did not subsequently have cholecystectomy. Among 450 patients, recurrence of biliary events occurred in 11% over a median follow-up of 36 months. Acute cholecystitis was the most common event, and very few patients required surgery or endoscopic intervention, with no operation-associated mortality or morbidity.
There Is No Such Thing as Too Soon: Long-Term Outcomes of Early Cholecystectomy for Frail Geriatric Patients with Acute Biliary Pancreatitis.2 This study assessed frail geriatric patients (65 years or older) with acute biliary pancreatitis. The research compared outcomes between patients who underwent early cholecystectomy (CCY) at index admission and those managed non-operatively with endoscopic retrograde cholangiopancreatography (ERCP). Early CCY was associated with lower rates of complications, readmissions, and mortality compared to non-operative management. A significant proportion of patients under non-operative management subsequently required unplanned cholecystectomy, which was linked to higher complication rates and costs.
Debate
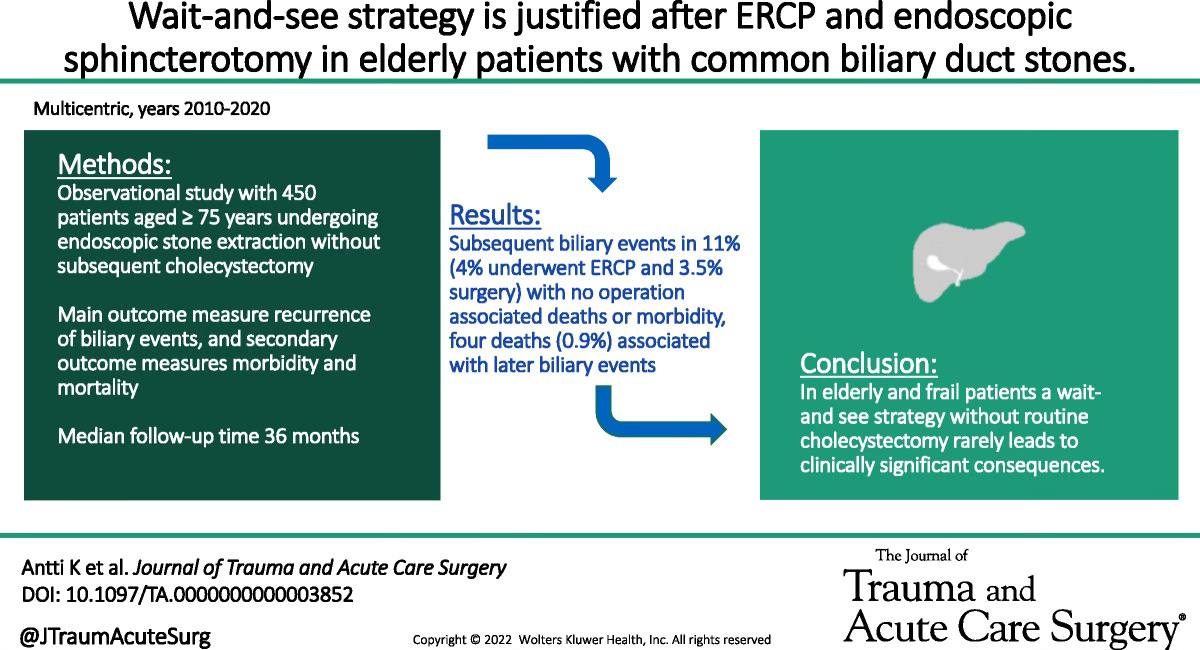
Position 1: Delayed Cholecystectomy After ERCP The first study presents a compelling argument for a wait-and-see strategy post-ERCP in elderly patients with common bile duct stones. The findings suggest that deferring cholecystectomy after successful stone removal is relatively safe and rarely results in severe consequences. With only a small fraction requiring later interventions and no adverse outcomes, this approach advocates for a conservative stance, especially in the elderly and frail demographic.
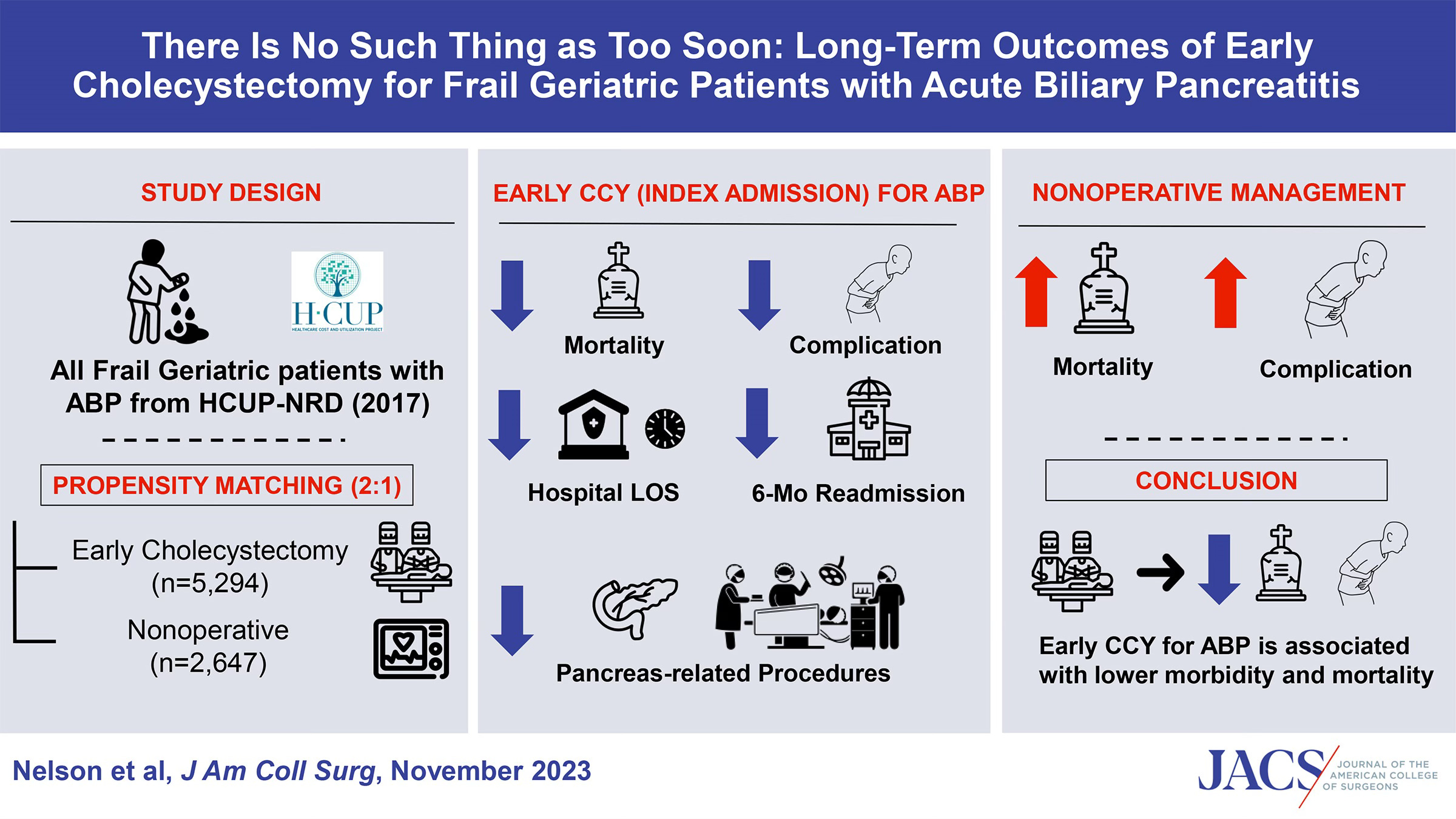
Position 2: Advocating for Early Cholecystectomy in Frail Geriatric Patients Contrary to the wait-and-see approach, the second study emphasizes the merits of early cholecystectomy, particularly in frail geriatric patients with acute biliary pancreatitis. It highlights the superiority of early surgical intervention in reducing complications, readmissions, and mortality rates compared to non-operative management with subsequent unplanned cholecystectomy. The data support the notion that postponing surgery in such patients might lead to poorer outcomes and higher healthcare costs.
Conclusion
The debate on the optimal timing of cholecystectomy in elderly and frail patients post-ERCP is intricate and multifaceted. While one study advocates for a watchful waiting strategy, emphasizing the infrequent need for intervention and acceptable outcomes without immediate surgery, the opposing study strongly favors early cholecystectomy, emphasizing the risks of delaying surgery, higher failure rates of non-operative management, and subsequent adverse outcomes.
Both studies highlight limitations: the first might downplay the significance of delayed cholecystectomy in certain subgroups, and the second might not account for varied patient presentations or risks associated with immediate surgery in frail individuals. The debate underscores the complexity of patient management decisions, urging a nuanced approach that carefully weighs individual patient factors, potential risks, and benefits of surgery versus conservative management. In conclusion, personalized patient care remains pivotal, necessitating a patient-centered approach grounded in sound clinical judgment and a comprehensive evaluation of each patient's unique circumstances.
Kivivuori, A., Mattila, L., Siiki, A., Laukkarinen, J., Rantanen, T., & Ukkonen, M. (2023). Wait-and-see strategy is justified after ERCP and endoscopic sphincterotomy in elderly patients with common biliary duct stones. The Journal of Trauma and Acute Care Surgery, 94(3), 443–447. https://doi.org/10.1097/ta.0000000000003852
Nelson, A. C., Bhogadi, S. K., Hosseinpour, H., Stewart, C., Anand, T., Spencer, A. L., Colosimo, C., Magnotti, L. J., & Joseph, B. (2023). There is no such thing as too soon: Long-term outcomes of early cholecystectomy for frail geriatric patients with acute biliary pancreatitis. Journal of the American College of Surgeons, 237(5), 712–718. https://doi.org/10.1097/xcs.0000000000000790